文献名: Discovery and saturation analysis of cancer genes across 21 tumour types.
我们知道对一个癌症的多个样本进行研究,其实很少高达20%样本突变 most intermediate frequencies (2–20%),还有很多低频突变,因为研究样本不够,从而不被发现
我们从 4,742个tumor-normal pairs的外显子测序数据集研究了somatic point mutations,共21种癌症。
癌症基因可能集中于以下七个功能:
proliferation,
apoptosis,
genome stability,
chromatin regulation,
immune evasion,
RNA processing
protein homeostasis
我们用有放回的抽样方法对数据进行统计,得出结论:如果我们对某个癌症的研究样本高达500-6000个的话,可以发现更多的临床低频突变。
这篇文章是为了解决以下三个问题:
1、大规模的研究cancer就能达到鉴别出所有的cancer driver genes的程度吗?(Coverage of known cancer genes)
2,增大样本量是否会揭示很多cancer driver genes?(Analysis of novel candidate cancer genes)
3、我们距离对所有的cancer driver genes的完全认知还有多远?(Saturation analysis)
突变数据的分析流程是Broad’s stringent filtering and annotation pipeline
突变情况如下:
3,078,483 somatic single nucleotide variations(SSNVs),
77,270 small insertions and deletions (SINDELs)
29,837 somatic di-, tri- or oligonucleotide variations (DNVs, TNVs and ONVs, respectively)
an average of 672 per tumour–normal pair
包括:
540,831 missense,
207,144 synonymous,
46,264 nonsense,
33,637 splice-site
2,294,935 non-coding mutations
我们找驱动基因的方法是:
We used the most recent version of the MutSig suite of tools
which looks for three independent signals:
high mutational burden relative to background expectation,
accounting for heterogeneity;
clustering of mutations within the gene;
enrichment of mutations in evolutionarily conserved sites.
我们把以上MutSig的几个独立组件分析得到的p-value组合起来,判断驱动基因,我们即对每种癌症做了单独分析,同时也对这21种癌症做了综合分析。
我们找到的驱动基因的结果:
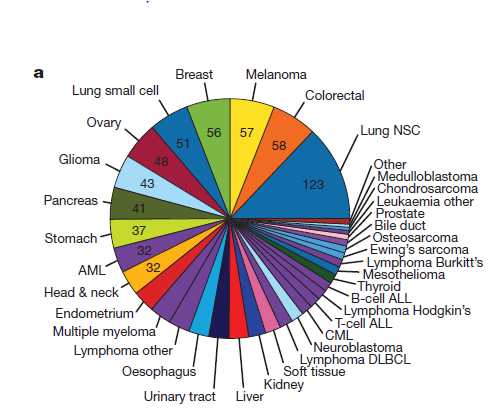
单独对各个癌症进行分析,可以总共找到334个基因,当然不同癌症找到的基因有交集。
These 334 pairs involve 224 distinct genes.
The number of genes detected per tumour type varied considerably (range of 1–58)
找到的驱动基因的个数差异主要取决于癌症种类的不同,然后,跟该癌症的样本量有关。
只有22种基因能在超过三种癌症里面都是被判定为驱动基因。
如果我们把21种癌症合并起来找驱动基因,可以找到114个,其中有30个是单独对各个癌症进行分析所找不到的,有80个在单独癌症分析可以找到。
所以单独对各个癌症进行分析找到的224个基因里面,有140个是合并癌症分析找不到的。其实画一个韦恩图就很好理解了。
对各个癌症进行分析,共21次分析,加上合并分析,共22次飞行,总共可以得到a Cancer5000 set containing 254 genes.
我们再严格分析一下254个基因在Cancer5000 set,得到219 distinct genes.叫做Cancer5000-S (for ‘stringent’) gene。
Cancer Gene Census (CGC)组织的 (v65)版本包含着130个cancer genes driven by somatic point mutations,其中82个被我们这次统计分析发现啦。
Four genes encode anti-proliferative proteins, in which loss-offunction mutations would be expected to contribute to oncogenesis.
Sixadditionalgenesencode proteins thatare clearlyinvolved incell proliferation: RHEB, RHOA, SOS1, ELF3, SGK1 and MYOCD.
Five genes encode pro-apoptotic factors, in which loss-of-function mutations would be expected to promote oncogenesis
Six genes encode proteins related to genome stability.
Fivegenesareassociatedwithchromatinregulation
Three genes encode proteins whose loss is expected to help tumours evade immune attack
Three genes are associated with RNA processing and metabolism.
One gene, TRIM23, is involved in protein homeostasis.
Beyond these 33 genes, the set of 81 novel genes is likely to contain
additional true cancer genes.
有返回抽样方法是:An effective test is to perform ‘down-sampling’; that is, to study how the number of discoveries increases with sample size, by repeating the analysis on random subsets of samples of various smaller sizes.
饱和度分析结果: 还远未到饱和,不同突变频率的基因被发现的个数随着样本量的增大而增多的速度不同。
Genes mutated in 20% of tumours are approaching saturation;
those mutated at frequencies of 10–20% are still rising rapidly, but at a decreasing rate;
those at 5–10% increasing linearly;
and those at ,5% are increasingly at an accelerating rate.
我们对样本量的要求是:突变背景高的癌症(如,黑色素瘤)需要的样品更多,而那些突变背景低的癌症(如成神经细胞瘤)需要近650个样本就可以很好的分析驱动基因了
Creating a reasonably comprehensive catalogue of candidate cancer genes mutated in 2% of patients will require between approximately 650 samples (for tumours with ,0.5 mutations per Mb, such
as neuroblastoma) to approximately 5,300 samples (for melanoma, with 12.9 mutations per Mb)